|
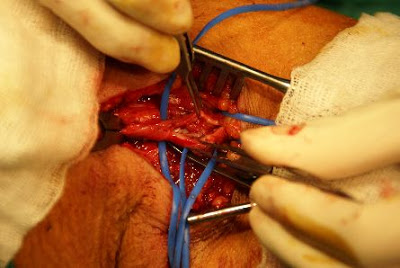
Dialysis graft outelt stricture is one of the most frequent complication/situation that a dialysis surgeon faces in his dailiy practice. To cope with the stenotic lesion, the oldest way, probably the most reliable, is to do surgical revision. There are two ways of surgical revision of the graft outlet. Here shows the so called" patch angioplasty" method. If the stenotic lesion is a focal or short lesion, we can just longitudinally incise teh graft outlet, and apply a ePTFE patch (which is the same material of the graft) to augment the outelt space. after the operation, the graft outlet should be widely open. The operation usually takes around 1 hour to perform. ofcourse, reoperation sometimes will be troublesome. However, most of the stenotic lesion can be fixed by patch angioplasty. Only if the lesion is too long, then we will try to fix the lesion using a jump graft. Ofcourse nowadays most of the graft outelt stenotic lesion are first treated with angioplasty balloons/ stenting, which is less invasive. However, surgeon should always keep himself familiar with the open procedure. and once the PTA doesnt work, we still can provide a feasible choice of treatment instead of giving up the graft! 
0 Comments
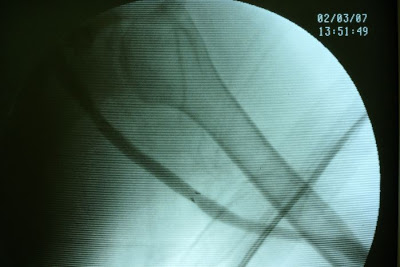
History A patietn of ESRD on regular dialysis vie her left upper arm graft. graft outlet segmental stricture was noted and the stenosis was refratory to repeated PTA (percutaneous balloon angioplasty). Operative finding During the venography study, graft outelt segmental stricture was noted. Due to the elasticity of the stricture, definite treatment is needed. Strategy Definite repair of the outlet stricture was needed. The options were: 1. Surgical revision, which is more invasive and time consuming. In addition, the lesion extended up to the high axillary vein make the revision more difficult. General anesthesia was needed to do the jump graft revision which will add on more anesthesia risk. 2. PTA with stent insertion. Covered-stent insertion over the stricture segment can prohibit immediate recoil and may prevent recurrent stricture in the long run. In addition, it's only a percutaneous procedure which is low risk to the patient. Thus we had proceed with covered-stent implantation to deal with the graft outlet recurrent stricture. 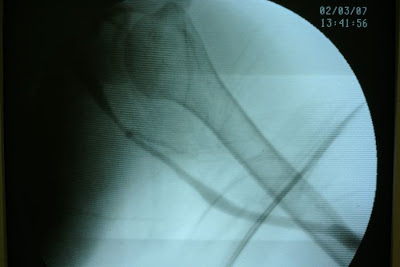
|
Blog by a
Vascular surgeon in Taiwan AuthorPo-Jen Ko MD Archives
February 2024
Categories |
 RSS Feed
RSS Feed
Copyright © 2014-2024 by Po-Jen Ko